8% of all intracranial space occupying lesions (SOL).
About one sixth as frequent as bacterial meningitis
0.7% of all neurosurgical operations
Source of infection-
Contiguous suppurative focus
Direct extension through osteitis /osteomyelitis/ meningitis
Retrograde thrombophlebitic spread via diploic /emissary veins
Local lymphatics
Post trauma (3-17.2%)
Hematogenous spread from a distant focus
Cryptogenic origin
Miscellaneous
Stages of abscess formation:
1 Early Cerebritis:
Perivascular inflammation, characterised by Neurutrophils infiltration and some swelling around infection site.
From Days 1-3
Late cerebritis:
A central area of necrosis develops as the surrounding oedema progresses. There is accumulation of fibroblasts around it
From Day 4-9
Early Capsule:
Establishment of a ring-enhancing capsule of Well-vascularised tissue with further fibroblast migration
Day 10-14
Late Capsule:
Collagen fibres and granulation tissue deposits leading to thickening of capsule effectively walling off the areas from surrounding brain.
Day 15 and beyond
Medical treatment-
Antibiotics- Chloramphenicol, Metronidazole, Sulphonamides, Isoniazid, and Rifampin which penetrate well into normal brain and CSF.
Staphylococcal brain abscess has shown that the penetration of Vancomycin is excellent; concentration of Vancomycin in the abscess fluid was found to be 80% of the simultaneously obtained serum concentration.
Pre-operative use of antibiotics would prevent the spread of infection during aspiration or surgical removal of the abscess.
Selection of antibiotics pre-operatively will be based on the etiology of an abscess and organisms most frequently encountered.
Later on, after obtaining the culture and sensitivity, proper antibiotics should be started.
The antibiotics most commonly used are cefotaxime, vancomycin and metronidazole.(effectiveness was 88%)
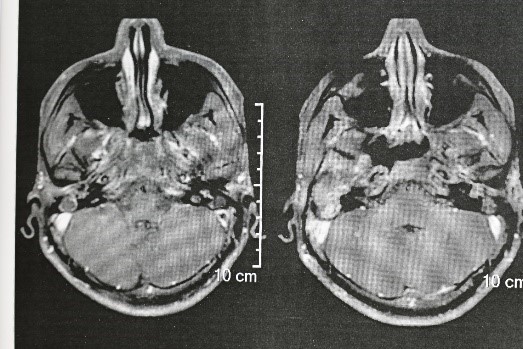
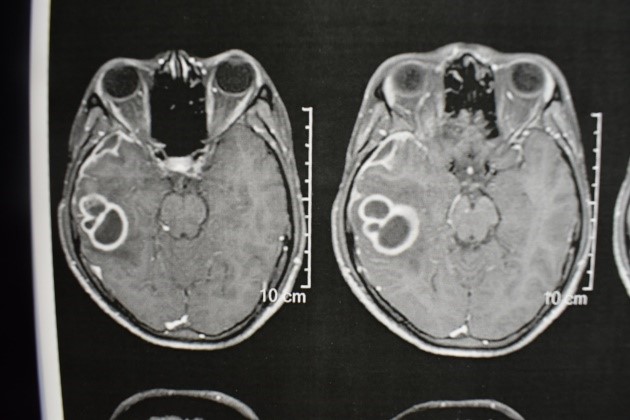
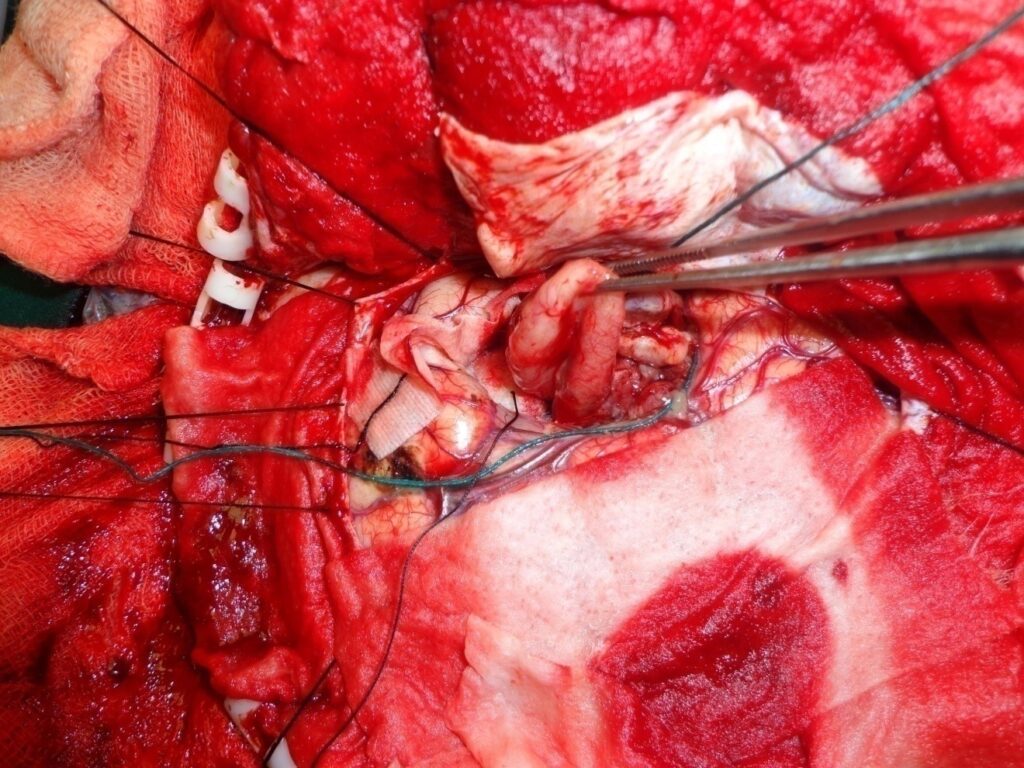
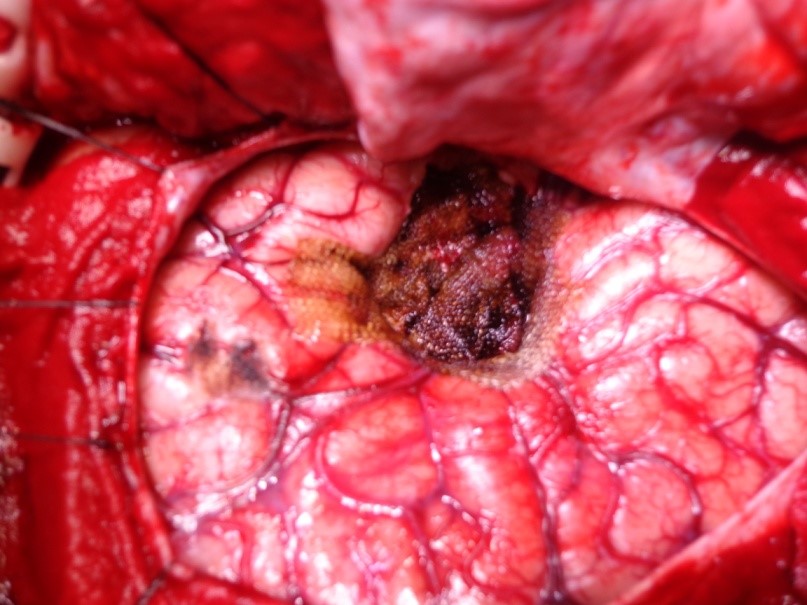
Brain abscess from right ear infection-
12 years / M
Known patient of right ear pus discharge
Headache, fits and fever
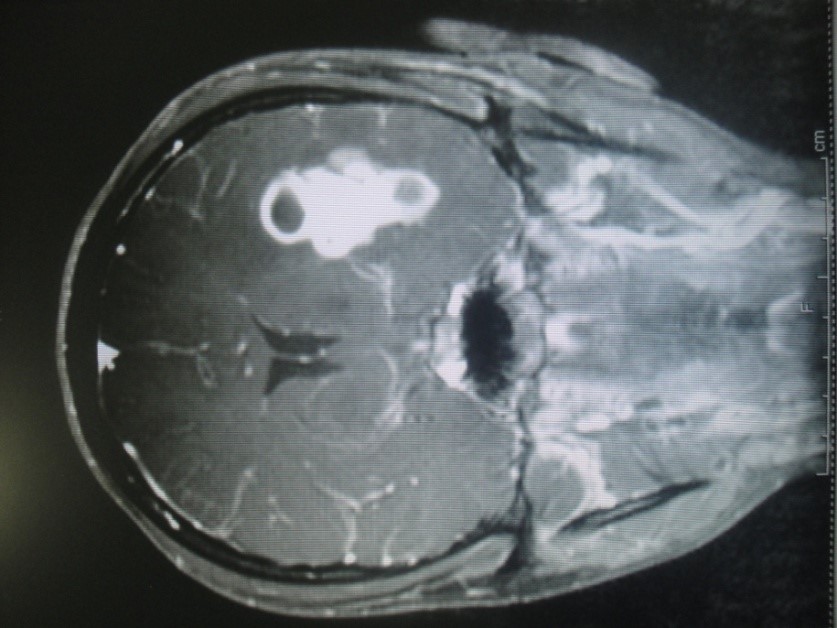
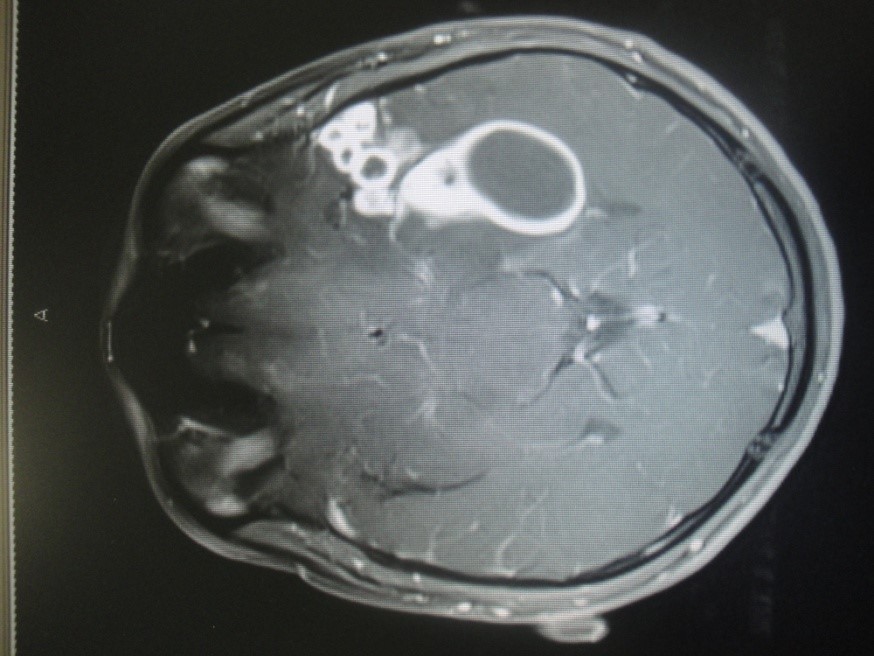
MRI Brain showed Right Temporal abscess with right side mastoiditis. (Fig 1 and 2)
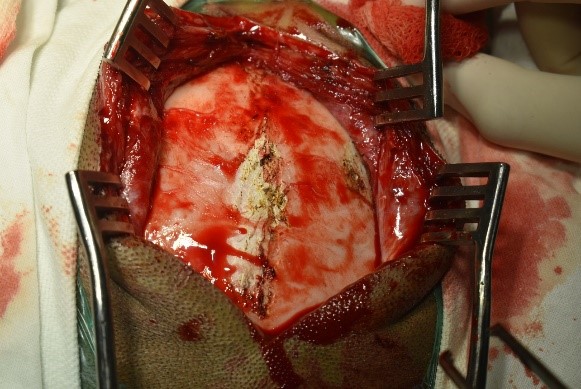
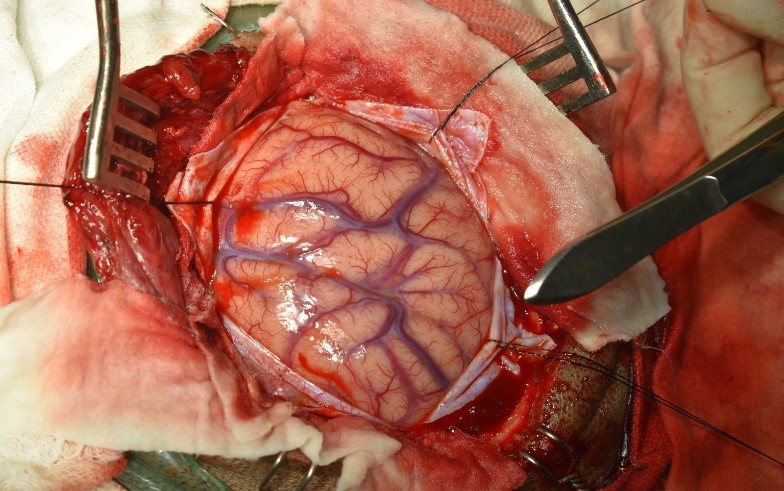
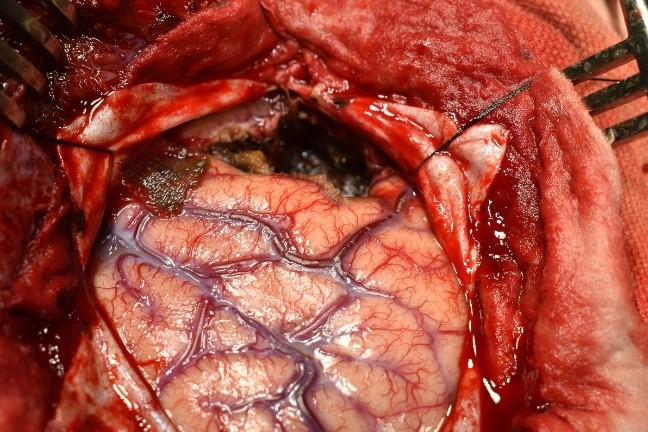
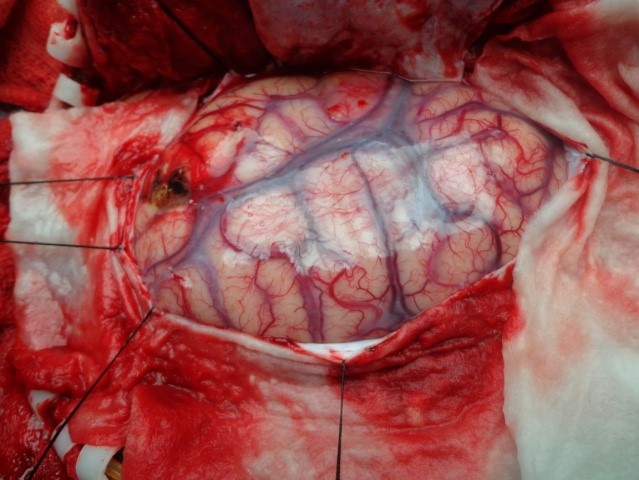
Underwent craniotomy and excision of the abscess (Fig 3-7)
Tubercular Brain abscess
26 M, CA
CNS Kochs
3 yrs of Antikochs, initially responsive later resistant
MRI Brain plain and contrast showed multiple left peri-sylvian Tuberculous abscesses. (Fig 1-3)